For decades the diagnostic of prostate cancer has relied on a triad based on a clinical examination by digital rectal examination (DRE), a blood test with a prostatic specific antigen (PSA) and an imaging by transrectal ultrasound scan (TRUS).
• The digital rectal examination
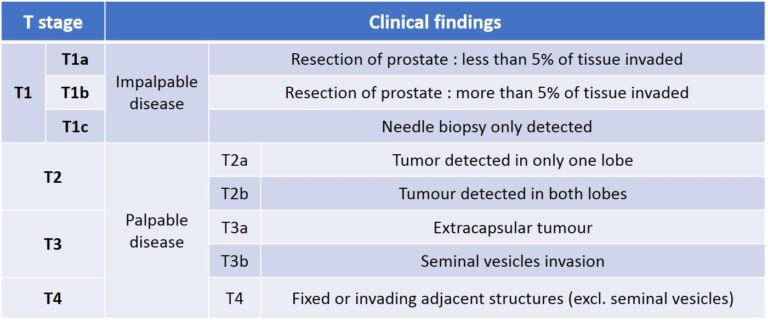
Long before any other diagnostic test, the DRE has been the only way to detect prostate cancer. It allows to evaluate 33% of the prostate surface. The DRE is recommended by all the learned societies even if a meta-analysis on more the 8000 studies on the subject concluded that given the considerable lack of evidence supporting its efficacy it should not be recommended to perform routinely a DRE to screen for prostate cancer in the primary care (picture 16a) setting [8]. When a cancer is detected by DRE in 50% of the cases it has already move beyond the limit of the prostate. In oncology, the TNM (tumour – nodes – metastasis) classification is the core of the staging of any cancer. In prostate cancer the T is clinical and determined only by the DRE (table 1 and picture 16b).
Picture 16 a : Digital rectal examination on a sagittal anatomical view (by B. Batard)
Table 1 : The tumour (T) parameter of the TNM classification of prostate cancer
Picture 16 b : Presence of the tumour into the prostate according to the T stage
• PSA molecule
First characterised in the 70’s by Dr Richard Ablin for the purpose of rape conviction, the raise of PSA has been associated with prostate cancer in 1981 (picture 17). It is produced by the glandular cells either normal, hyperplastic or cancerous. Its concentration increases with age (table 2), presence of a benign prostatic enlargement, a cancer or an inflammation of the prostate called prostatitis from infectious origin or else. PSA is definitely not a tumour marker as every man with a prostate will have a certain concentration of PSA in his blood test. Even if the PSA has been criticized for its inaccuracy it is still necessary as a first step diagnosis (table 3).
Picture 17 : 3D molecular structure of the Prostatic Specific Antigen (PSA)
Eventually there are many other derivatives to the PSA such as ProPSA, cPSA, BPSA, sPSA-N, Intact PSA, PSADT, PSAphi….
Table 2 : Acceptable range of PSA related to age
Many derivates of the PSA have been proposed :
PSA free/total
- Free form constitutes 5-40% of total PSA
- If the PSAF/T is below 0.1 there is an increased risk of PCa
PSA velocity
– Represents the annual absolute increase in total PSA
– when PSA levels 4-10 ng/mL the acceptable increase is below 0.75 ng/ml/year
PSA density
– The PSA density (PSAD) is the ratio PSA/prostate volume knowing that the production of PSA varies depending on type of prostatic tissue :
• normal prostate epithelium = 0.1 ng/mL
• BPH = 0.3 ng/mL
• PCa tissue = 3.5 ng/mL
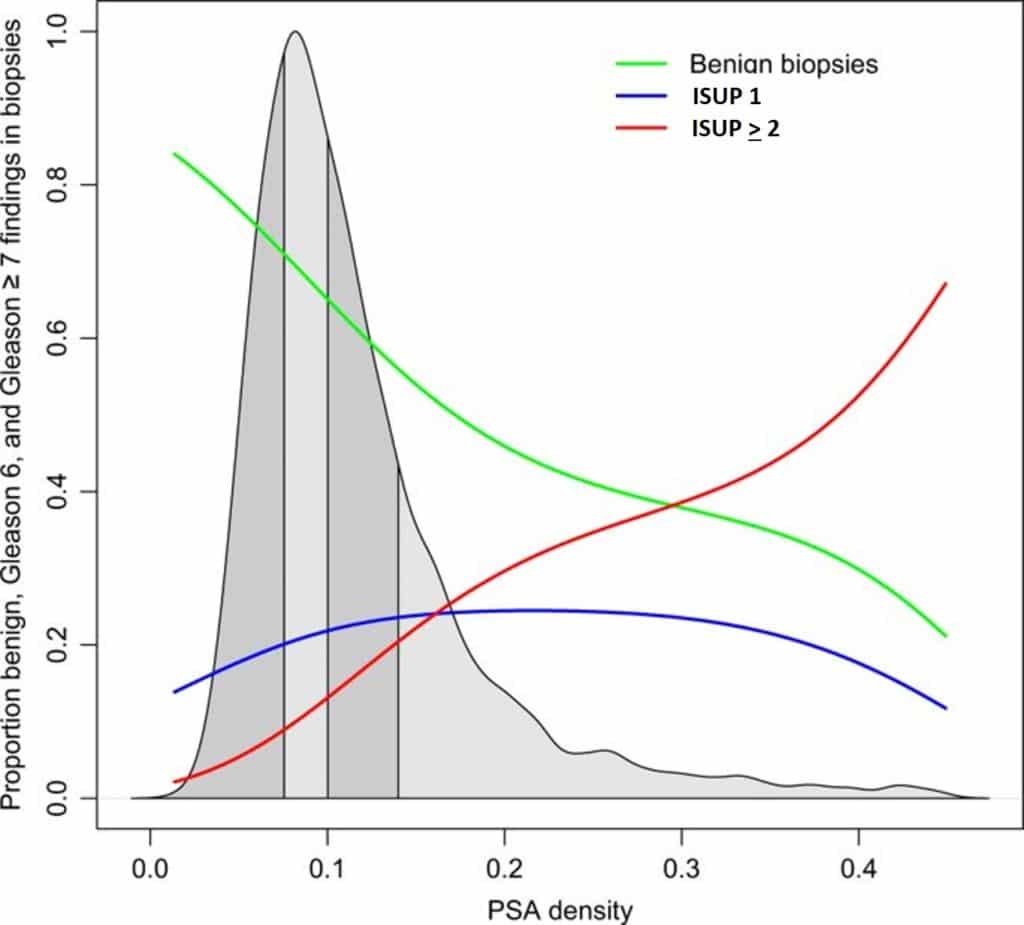
– Therefore when the PSAD is above 0.15 the risk of prostate cancer is increased (figure 1)
– Conversely when the PSAD is below 0.1 the risk of prostate cancer is very low and it avoids to perform a new set of biopsies in 31% when the first set was already negative [9].
Figure 1 : Proportion of benign, ISUP 1 and ISUP > 2 related to PSAD
Table 3 : Probability of prostate cancer according to PSA blood test (source : EAU guidelines 2020)
• Transrectal ultrasound
The transrectal ultrasound scan (TRUS) has been described as early as 1968 by Watanabee et al. It is the best way to visualize the prostate by introducing the US probe into the rectum. The prostate being just in the front of the anterior rectal wall it gives a nice image of the prostate without any interference (picture 18). It has an interest to make the most accurate measurement of the prostatic volume however TRUS has no direct diagnostic relevance has the vast majority of prostate cancer are invisible on US scan. Meanwhile TRUS is still essential to perform the prostate biopsies and also for the planning of minimally invasive treatment such as focal therapy.
Picture 18 : Transrectal ultrasound (TRUS) with the immediate proximity of the prostate to the US probe (by B. Batard)
Multiparametric Magnetic Resonance Imaging (mpMRI)
The multiparametric Magnetic Resonance Imaging (mpMRI) is the diagnostic milestone of this 2 last decades in the expertise of prostate cancer. Nothing has changed the way of managing prostate cancer as much as mpMRI in the diagnostic as much as in the therapeutic field. Except for an obvious metastatic prostate cancer at its first presentation, no prostate cancer should be managed without a high-quality mpMRI.
The prostatic biopsies (PB) are the cornerstone of any prostate cancer treatment decision making. The technical improvement in the way of taking prostate biopsies has been revolutionized by the surge of mpMRI in the field. In the vast majority of the cases, the technology of fusion biopsy should not be anymore an option but an obligation as the accuracy brought by this new technology plunges prostate cancer management in the era of the 21th century.
With all these new knowledge and technologies now available no expert center would continue to diagnose and to treat prostate cancer as usual. The difference between a prostate cancer expert institution and a standard center does not rely anymore in the way you treat but rather how you diagnose patients. Indeed diagnostic accuracy has become the key element in every PCa management.
Overdiagnosis and overtreatment
Prostate cancer is the most frequent cancer in male during a lifetime.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Any cookies that may not be particularly necessary for the website to function and is used specifically to collect user personal data via analytics, ads, other embedded contents are termed as non-necessary cookies. It is mandatory to procure user consent prior to running these cookies on your website.