

Everything you need to know about prostate cancer
Prostate Cancer > Clinical scenarii
In the diagnostic workup, what really matters ?
The biopsy pathological results
In terms of cancer aggressivity and spread, the most important parameter is the result of the biopsies as it leads the prognosis.
- Aggressivity of the disease
The aggressivity of the cancer is based on the ISUP (International Society of Urological Pathology) classification which goes from 1 to 5. It has simplified the previous Gleason grading scoring with an easy concordance between the 2 systems (table 5)
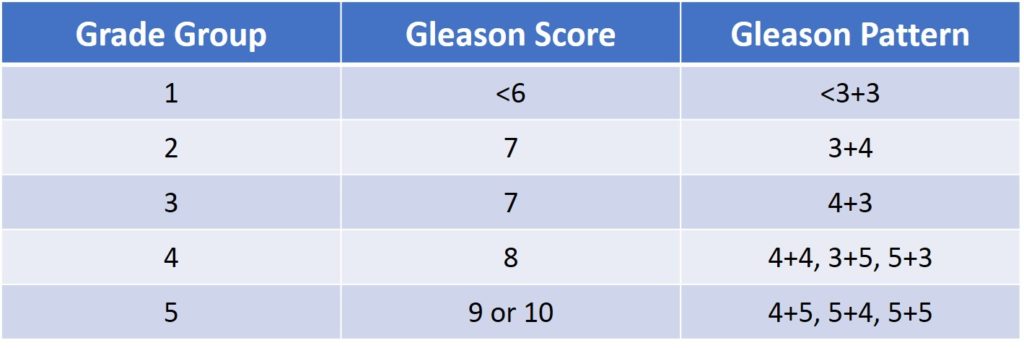
Table 5 : ISUP prostate cancer grade groups in correlation with the Gleason score grading
- Number of positive biopsies invaded
Depending on the number of cores invaded by the cancer it is possible to extrapolate how important is the cancer extension in your prostate. The more number of cores are involved the bigger your cancer is supposed to be. However if the number of cores taken is more important than needed it may appear artificially that your cancer seems important where merely the positive cores have being taken repeatedly in the same location.
- Length of cancer on each biopsy
The invasion length in each core is also a very important parameter to assess accurately the importance of the disease. Usually it is mentioned in the pathological report either in percentage or simply in millimetre. When the cancer is graded ISUP 1 or sometimes even ISUP 2, in some learned societies guidelines the threshold of 3 mm matters as above this invasion length the risk of progression is more asserted.
The multiparametric MRI report
In the recent years it has become a central point to any prostate cancer management at such level that the most important learned societies have made the mpMRI examination mandatory before any prostatic biopsy procedure.
- Importance of the lesion(s) size
The mpMRI is able to detect lesion as small as 5 mm or sometimes even less. The more agressive is the cancer the easier is the detection on mpMRI with a degree of suspicion express by the PI-RADS classification (table 4). Even if the most accurate assessment would be to get the volume of each lesion most of the time the evaluation of each lesion is expressed by the length of the bigger axis of the lesion.
- Capsule
The description of the capsule is fundamental because it separates the prostate cancer between organ-confined and extra-capsular disease. Regarding the tumour staging in one case the cancer is strictly localized to the prostate with all the therapeutic consequences of such situation and in the other case the locally advanced aspect of the disease de facto excludes some therapeutic options.
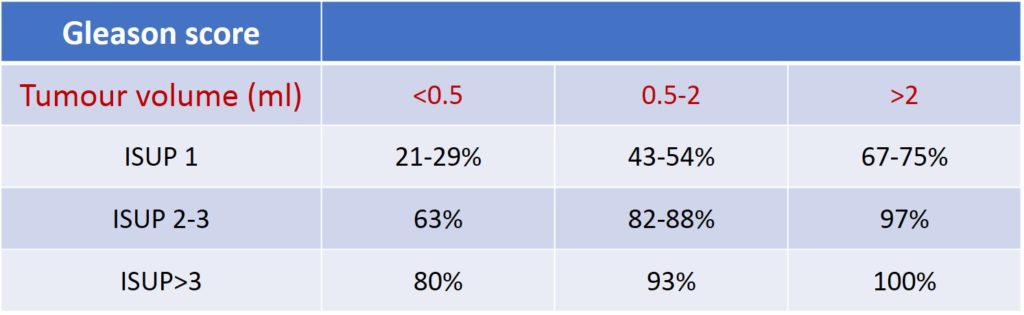
Table 4 : prostate cancer detection rates by mpMRI based on tumour volume and ISUP classification
The 3 different clinical scenarii
The classification of prostate cancer in different groups has been largely improved by the scientific studies of Pr A. d’Amico. Based on the digital rectal examination, the PSA blood test and the Gleason score grading (now ISUP) it allows to separate the prostate cancer patients in 3 different groups of low, intermediate and high risk of recurrence after a radical treatment (picture 36) [10]. For the time being, even if insufficiently accurate the d’Amico classification is the best tool available to assess the prognostic of a patient. An updated d’Amico classification has been proposed (see « Prognosis and follow-up »)
- Low risk prostate cancer
Actually it represents around less than 20% of the cases and low risk (LR) is in the context undoubtely the best situation one can expect. A LR situation is mostly clinically irrelevant with a limited risk of progression. In 2013, the Popiolek study has shown that the risk of death after 23 years of follow-up is around 1 out of 10 patients which at a certain age is a very limited risk. In that situation, a follow-up is still needed but with a very weak risk of cancer spread and by keeping in mind that time is your best ally and any fast management is at least a mistake. When a prostate cancer is classified as LR the unit of time is neither the week or the month but rather the year.
- Intermediate risk prostate cancer
The intermediate risk (IR) is the grey zone of the spectrum with a potential of progression. With the ISUP classification it has been divided in 2 different groups where the « favourable » IR includes only the ISUP 2 with short a limited number of cores invaded and a short distance of cancer in each core. This field needs further studies however with less than 50% cores invaded with less than 20% grade 4 on each positive core the patient may be considered as favourable IR.
Very close to the LR favourable IR presents a limited risk of death but possibly a metastatic issue. In this respect, the evaluation of life expectancy and its impact on any therapeutic decision process should play a central role. To avoid a metastatic evolution a physical treatment may be needed either radical or focal.
When not favourable the IR presents an important risk of progression and there is no doubt that the cancer will grow. Your theoretical life expectancy is a still a major issue to decide whether a tight surveillance is sufficient or an eradication of the cancer is needed. In the latter case a physical treatment either radical or focal of the cancer aims to eradicate completely the disease or sometimes to sufficiently slow down the natural path of prostate cancer to avoid any complications or symptoms when not treated.
Even in IR situations sometimes poor parameters leave only the options of a radical treatment alone or within a multidisciplinary strategy.

Picture 36 : The d’Amico classification with the risk of recurrence
- High risk prostate cancer
High Risk (HR) represents the difficult cases. Without a very serious and sometimes aggressive therapeutic protocol, this dangerous group is a threatening-life situation at mid- or even short-term. A multidisciplinary management of your disease involving Urologists, Radiotherapists and sometimes Oncologists to slow down or defeat the cancer is absolutely needed. Even more than for the LR and IR patients an exhaustive staging workup is mandatory before any serious therapeutic proposition which will be taken during a weekly organized Multidisciplinary Team (MDT) meeting. Included in the staging workup any patient in this situation should have in addition to a previous mpMRI before the biopsies :
-
a Chest Abdomen Pelvis (CAP) CT scan to assess the presence or absence of nodal or visceral metastasis
-
A bone scan to assess the absence or presence of bony metastasis using the Tc99m MDP radionuclide. This nuclear medicine examination is not really sensitive and most of the time will show the bone lesions at an advanced stage.
-
A PET scan (Positron Emission Tomography) using the F18 FDG or in the best occurrence with the PSMA radionuclide aims to figure out bone as well as soft tissue metastasis. Unfortunately a F18 FDG-PET scan detects 30% false positive lesions overstaging the patient as metastatic (M+) while it is not the case. PSMA-PET scan is undoubtedly a far more reliable option with a high and accurate detection rate but still rarely available in most of the healthcare systems.
