Androgen deprivation therapy (ADT) in prostate cancer is the oldest systemic treatment available in the field of prostate cancer. It was published by C. Huggins in 1941 and won him the Nobel Prize for Medicine in 1966 (picture 73). It is based on hormone dependance of prostate cancer, where androgens are a vital fuel for the growth and progression of cancer cells. In male, androgens are produced by the testis for 95% and by the adrenal glands for the remaining 5%. The production of testosterone depends on the hypothalamus-pituitary gland axis, the former producing the luteinizing hormone-releasing hormone (LH-RH) which will induce the production of luteinizing hormone (LH) by the latter. LH stimulates the production of androgens by the testicles [Leydig cells] (picture 74). The hypothalamus controls the pituitary gland by intermittent secretions of LH-RH.
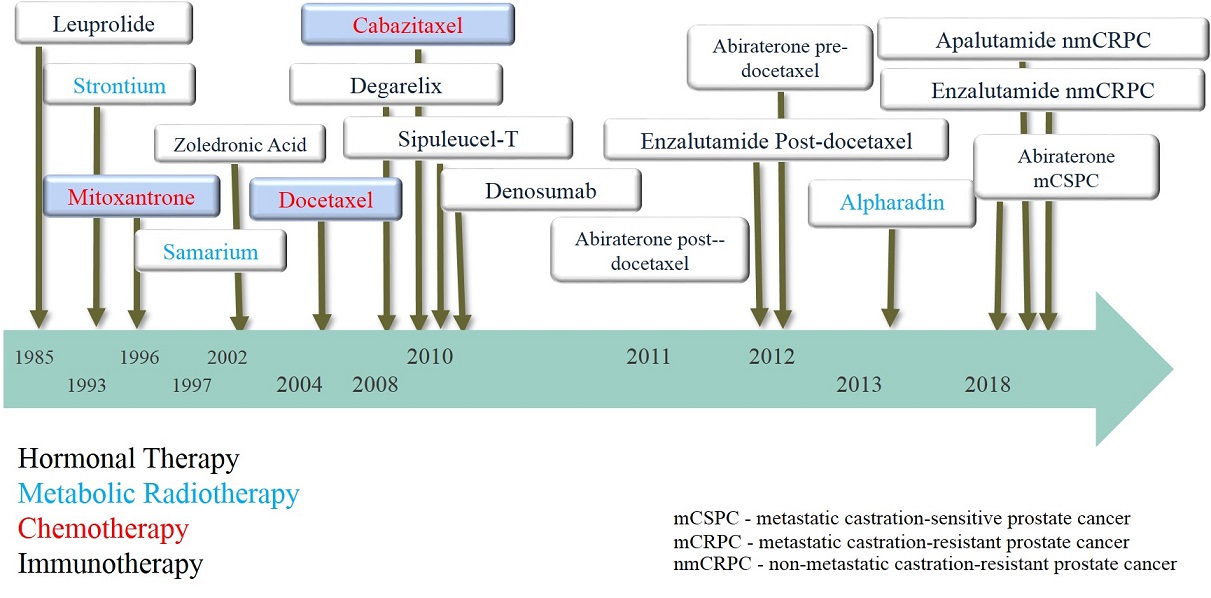
For a long time ADT was achieved only surgically by bilateral ablation of the testis (orchiectomy). Later in 1980 the first LH-RH (also called GnRH) agonist (i.e. leuprolide, goserelin or triptorelin) was used to obtain a chemical castration. The effect of the intramuscular injection lasted first 1 month then 3 months to reach 6 months after 2000. It could appear weird to inject an LH-RH agonist which naturally stimulates the production of androgens by the testis to obtain a hormonal deprivation. However the trick lies in the natural intermittent hypothalamic rythm of secretion of LH-RH which is completely broken by the injection and the continual diffusion of LH-RH instead. Beside the usual side-effects such as hot flashes, major sexual function impact, loss of muscle mass and fatigue, one of the disadvantage of LH-RH agonists is the flair-up at the initiation of the treatment. Indeed during the 2-3 first weeks the injection will rather increase the production of testosterone with a possible clinical progression of the disease. Usually to avoid the flair-up effect a complementary hormone treatment is given by adding anti-androgens (i.e. bicalutamide or flutamide) for the same period of time.