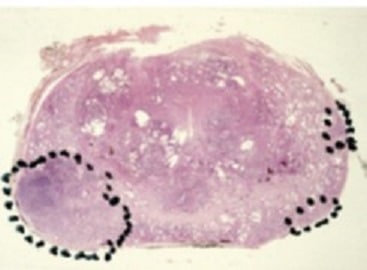
Prostate cancer is known to be multifocal in 80% of the cases meaning the presence of different lesions into the prostatic gland (picture 52). When multifocal different studies have shown the existence of one main lesion so-called the index lesion (picture 53). Studies have shown that the metastatic disease spreads from one cell contained in the socalled index lesion (picture 54) [20, 21]. The index lesion is the most important in volume representing 80% of the total tumour volume and is responsible for the spread of the cancer outside the prostate (extra-capsular extension) in almost 90% of the cases [22]. The index lesion is the most aggressive lesion it contains the highest ISUP score and therefore leads the prognosis of the disease. The destruction of the index lesion leaves one or several secondary smaller lesions less aggressive with a better controlled risk of metastatic evolution. Unlike radical treatments, focal therapy does not aim to completely eradicate the cancer but to bring the disease backwards and to take control of the remaining lifetime (video 6). With the high-resolution technology (mpMRI, fusion biopsies) already available today to control accurately any progression of the disease it is possible to consider at least Low Risk and favourable Intermediate Risk prostate cancer suitable for this innovative management. If a small lesion tends to grow it could be followed by active surveillance and when necessary the lesion will be targeted by focal therapy leaving behind smaller lesions. This scenario can be repeated endlessly with the perpetual improvement of technology and its increased accuracy.