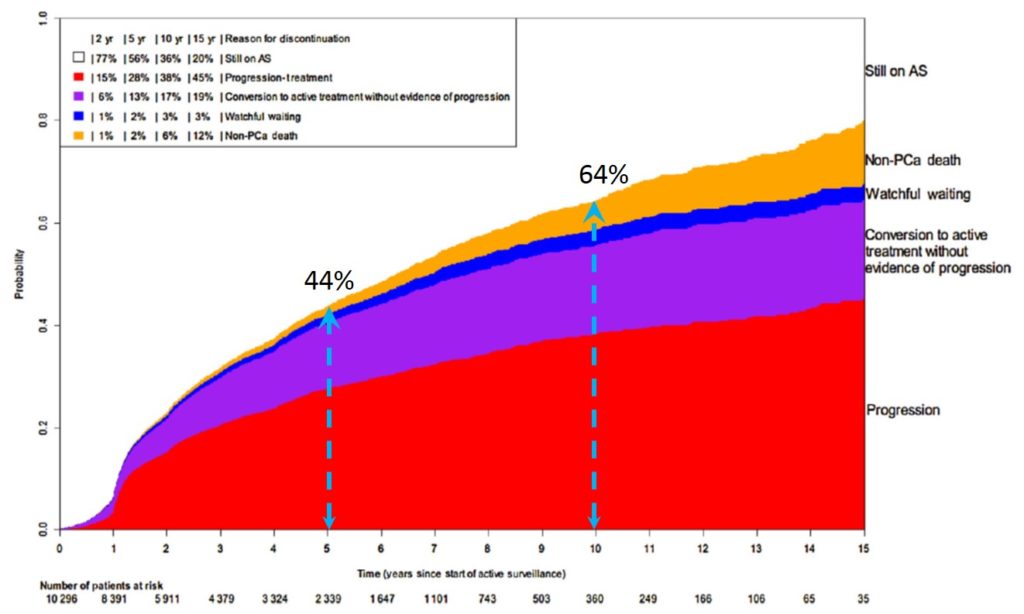
In the table 18, the number of patients who died from prostate cancer at 10-years follow-up is very low confirming the relevance of AS as a therapy in LR and selected favourable IR disease with the pitfall of progression. Indeed one-third of the patients within 2 years and around half of them at 5 years will progress. In the European PRIAS study, at 10 years follow-up, 73% of patients under AS decide to go for an active management often due to a more advanced disease [18]. Even in the Movember GAP3 Consortium population of more than 10 000 patients at 5 and 10 years respectively 44% and 64% of men engaged in an AS discontinued the strategy (picture 50) [19]. In order to get an optimal control of the potential spread of the disease at mid- or even long-term one would rather choose a physical treatment of his cancer when the cancerous lesions can still be easily destroyed.