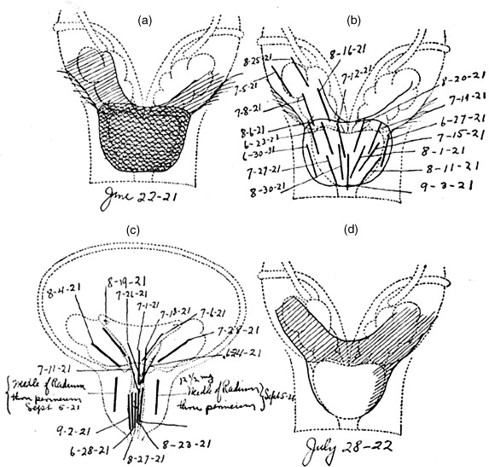
In 1911, a decade after the surge of the EBRT and radical prostatectomy, Dr O. Pasteau and P. Degrais, in Paris, initiated the use of internal radiation by positioning a source of radium inside an uretral catheter (picture 46). However it was Dr B. Barringer, in 1917, who was the first to place radium needles through the perineum (transperineal) into the prostatic gland opening the way to the modern interstitial brachytherapy (picture 47).